The complex relationship between keto and cholesterol: myths vs. reality
Evidence-based analysis of metabolic shifts and cardiovascular health.
In the realm of metabolic therapies, few topics generate as much controversy and clinical confusion as the relationship between keto and cholesterol. As a medical professional, I frequently encounter patients who have achieved remarkable weight loss and glycemic control on a ketogenic diet, only to be alarmed by a sudden shift in their lipid panel. The narrative surrounding dietary fat and heart health has evolved significantly over the last century, moving from a simplistic fear of all fats to a more nuanced understanding of lipidology.
However, the question remains: Does the high-fat nature of the ketogenic diet pose a threat to cardiovascular health? The answer is not a simple yes or no. While many individuals experience an improvement in their overall lipid profile—marked by lower triglycerides and higher HDL—a subset of patients sees a significant rise in LDL (“bad cholesterol”). Understanding why this happens requires a deep dive into physiology, the quality of dietary fats, and individual genetic variations.
This article provides an objective, evidence-based analysis of keto cholesterol interactions. We will dissect the myths, examine the latest research, and provide clinical strategies to maintain a heart-healthy profile while remaining in ketosis.
How keto affects cholesterol: the metabolic shift
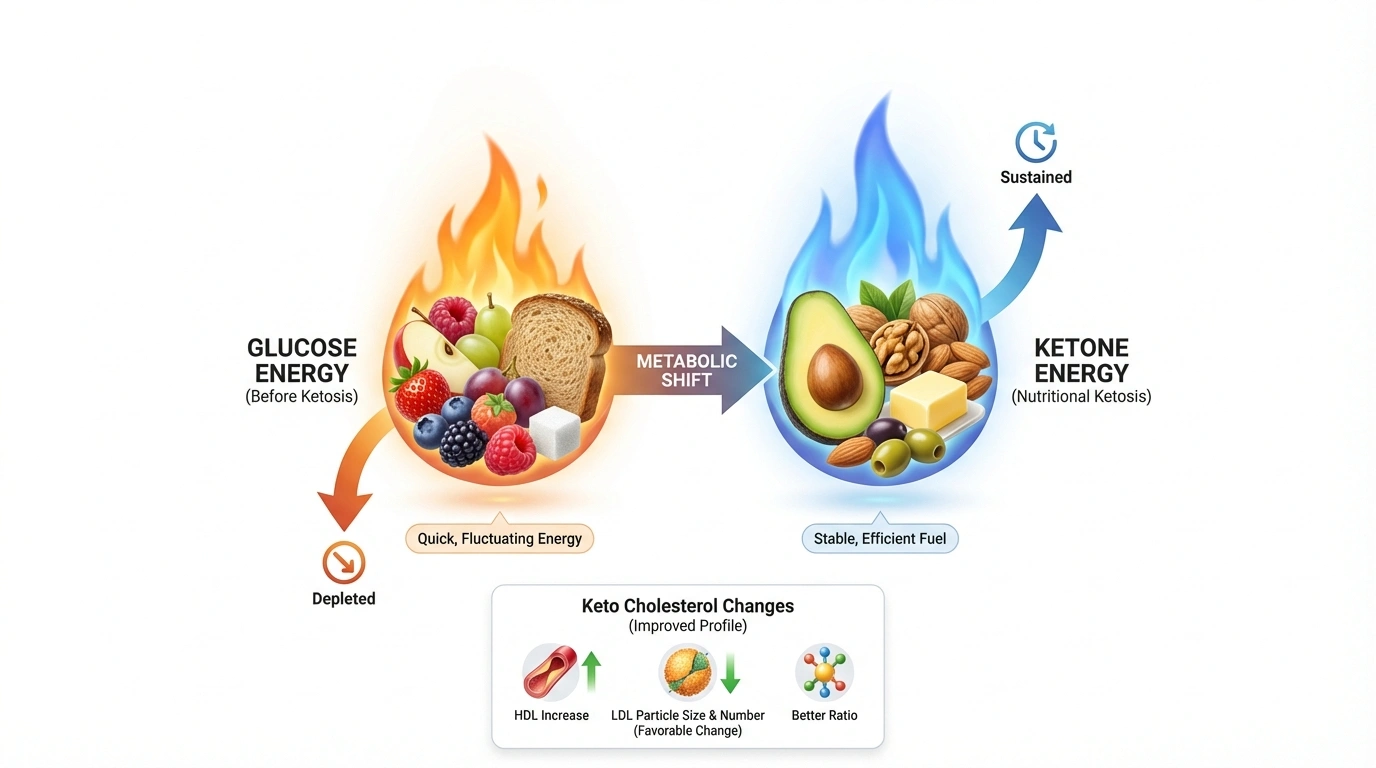
To understand the impact of keto cholesterol changes, one must first understand the fundamental metabolic shift that occurs during carbohydrate restriction. The standard ketogenic diet involves consuming approximately 70-80% of daily calories from fat, 10-20% from protein, and 5-10% from carbohydrates. This restriction forces the body to transition from using glucose as its primary fuel source to oxidizing fatty acids and ketone bodies—a state known as nutritional ketosis.
👇 Optimize Your Metabolic Profile
Establishing your boundaries is key to heart health on keto.
Estimated Daily Target
0
kcal / day
The standard lipid response
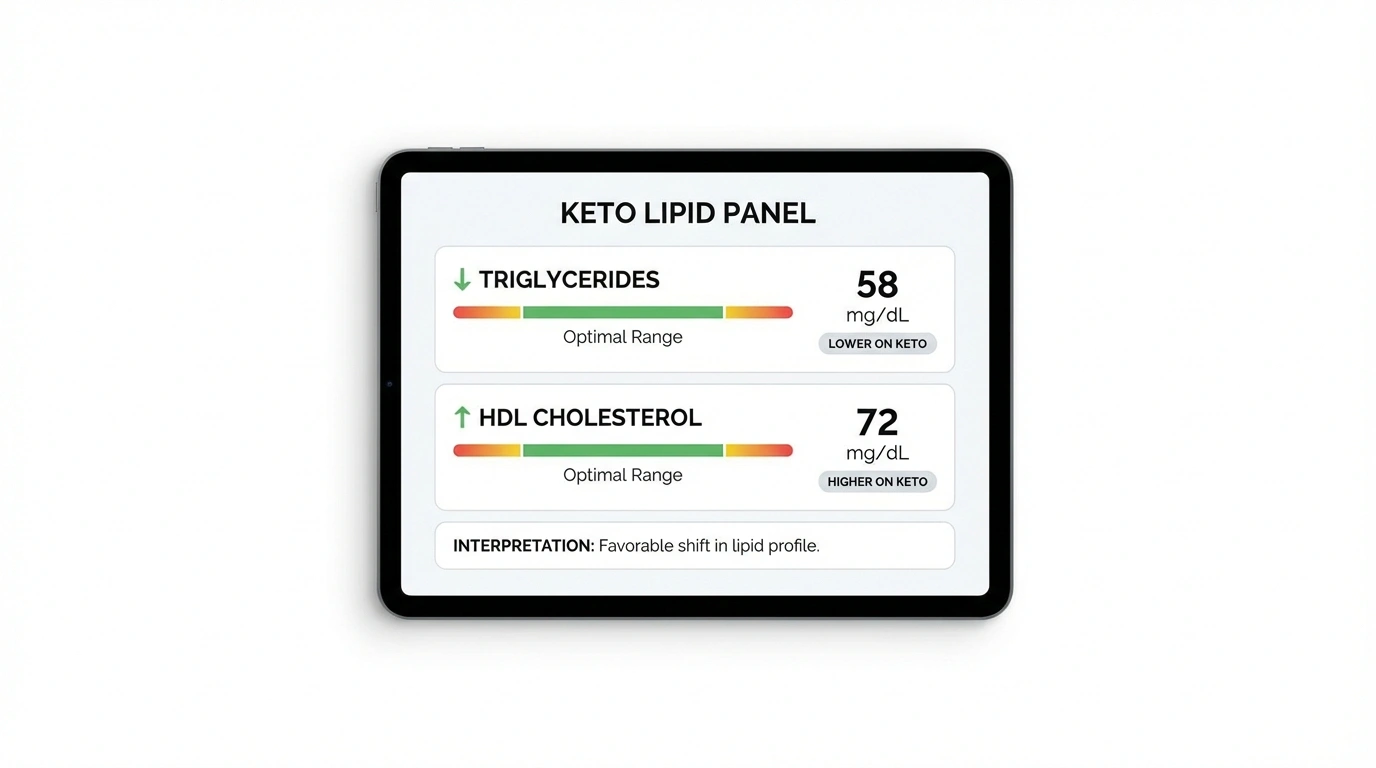
For the majority of patients with obesity or metabolic syndrome (insulin resistance), the ketogenic diet typically produces a favorable shift in specific lipid markers. Research consistently demonstrates the following trends:
- Reduction in triglycerides: high triglyceride levels are strongly linked to excessive carbohydrate intake and insulin resistance. When carbohydrates are restricted, the liver produces fewer triglycerides, and the body becomes more efficient at burning circulating fats for fuel. Studies indicate that low-carb diets are often superior to low-fat diets for lowering triglycerides.
- Elevation of HDL (high-density lipoprotein): often termed “good cholesterol,” HDL acts as a scavenger, transporting cholesterol from the arteries back to the liver for excretion. The ketogenic diet, particularly when rich in healthy saturated and monounsaturated fats, is effective at raising HDL levels.
- Variable impact on LDL (low-density lipoprotein): this is the area of greatest clinical concern. While triglycerides often drop and HDL rises, the response of LDL is highly variable. Some patients see a decrease or no change, while others experience a marked increase in LDL-C (total ldl cholesterol).
The nuance of LDL particle size
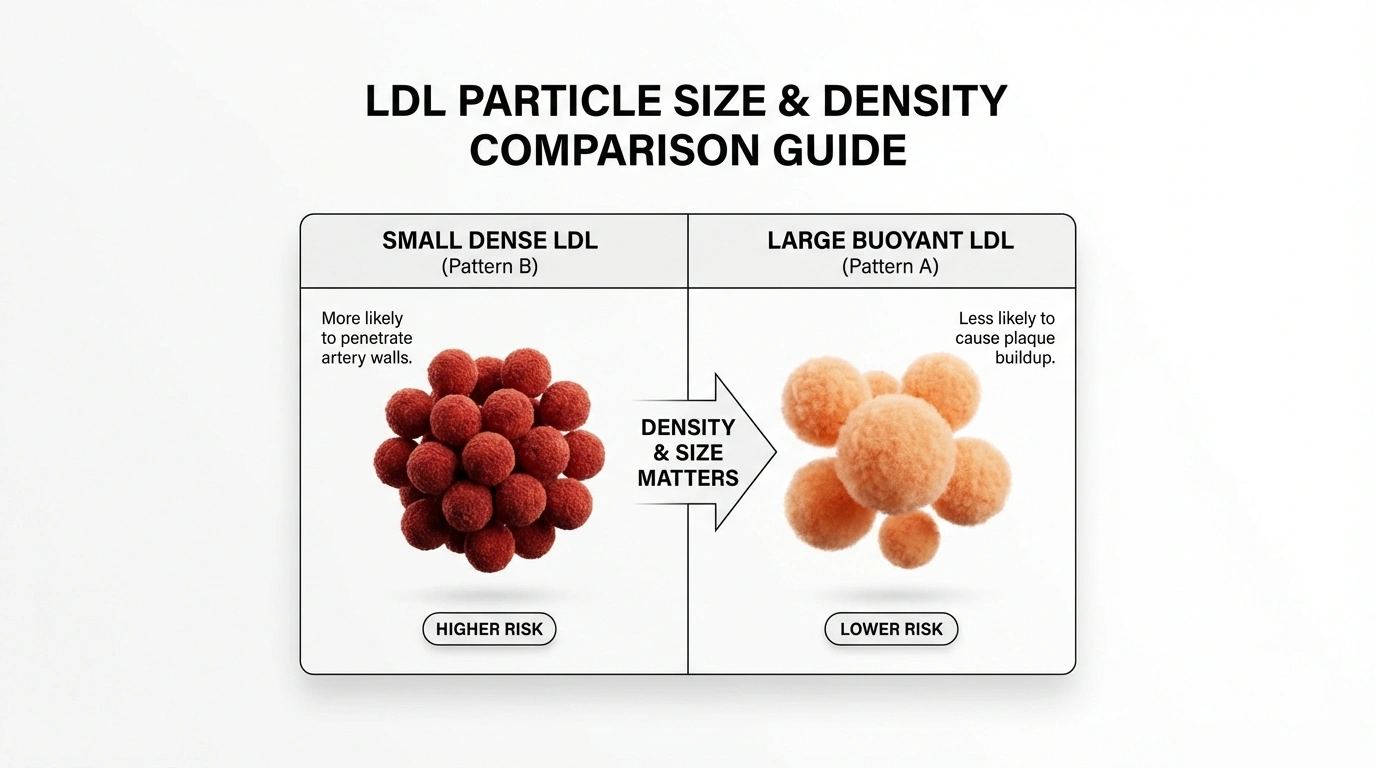
Standard lipid panels measure LDL-C, which is the total mass of cholesterol within LDL particles. However, this number does not tell the whole story. LDL particles vary in size and density:
- Small, dense LDL (pattern b): these particles are highly atherogenic, meaning they are more likely to penetrate arterial walls and cause plaque buildup (atherosclerosis).
- Large, buoyant LDL (pattern a): these particles are considered less harmful and are often associated with a lower risk of cardiovascular disease.
Carbohydrate restriction often induces a shift from pattern b to pattern a. Therefore, a patient might see their total keto cholesterol number (LDL-C) rise, but if the particle size has increased and triglycerides have plummeted, their overall cardiovascular risk profile may have actually improved. However, this is not a license to ignore extremely high LDL levels, as the total number of particles (LDL-P) and apolipoprotein b (ApoB) remain critical risk factors.
What the research says: analyzing the data
The medical community is currently debating the long-term safety of keto heart health outcomes. We must look at the data objectively, acknowledging both the benefits for metabolic syndrome and the potential risks of hyperlipidemia.
The case for improved cardiometabolic health
Numerous randomized controlled trials (RCTs) suggest that for patients with type 2 diabetes and obesity, the benefits of weight loss and glycemic control outweigh the risks of lipid alterations. A meta-analysis of RCTs found that low-carbohydrate diets were more effective than low-fat diets in reducing triglycerides and increasing HDL, while also significantly reducing body weight and blood pressure.
Furthermore, insulin resistance is a primary driver of heart disease. By lowering insulin levels and reversing metabolic syndrome, the ketogenic diet addresses a root cause of cardiovascular pathology. For many, the improvement in the triglyceride-to-hdl ratio (a powerful predictor of heart disease) suggests a protective effect.
The concerns: LDL elevations and ApoB
Despite these benefits, authoritative bodies like the National Lipid Association (NLA) have issued scientific statements advising caution. The NLA notes that while low-carb diets support weight loss, they are not universally superior long-term and may be contraindicated for patients with hypercholesterolemia, particularly those with genetic conditions like familial hypercholesterolemia.
A recent study utilizing data from the UK Biobank found that a “keto-like” high-fat, low-carb diet was associated with significantly higher levels of LDL cholesterol and apolipoprotein b (ApoB). More concerningly, this study observed a two-fold increase in cardiovascular events in the lchf group compared to those on a standard diet over an 11.8-year follow-up. It is important to note that this was an observational study, which shows correlation rather than causation, and dietary adherence was self-reported. However, it raises a flag that cholesterol on keto diet protocols cannot be ignored.
The “lean mass hyper-responder” (LMHR) phenotype
A fascinating phenomenon has emerged in the research regarding a specific subset of keto dieters known as “lean mass hyper-responders” (LMHR). These are typically lean, athletic individuals who adopt a ketogenic diet and see their keto cholesterol numbers skyrocket. The LMHR triad is defined as:
- LDL-C ≥ 200 mg/dL (often much higher)
- HDL-C ≥ 80 mg/dL
- Triglycerides ≤ 70 mg/dL
According to the “lipid energy model,” these individuals are not necessarily sick; rather, their bodies are trafficking massive amounts of energy (in the form of fat/triglycerides) via VLDL particles to lean tissues. As the triglycerides are stripped off for energy, the resulting particle is an LDL. Recent imaging studies (CCTA) on this group have shown that despite extremely high LDL levels, many LMHRs do not exhibit proportional plaque accumulation in the short term, though long-term data is still being gathered. This remains an area of intense research, and current guidelines still treat such high LDL as a risk factor.
The role of saturated vs. unsaturated fats
Why does one patient’s LDL remain stable while another’s rises? The answer often lies in the type of fat consumed. The macronutrient composition of a ketogenic diet can vary wildly. One person may consume “dirty keto” (bacon, processed cheese, butter), while another consumes “mediterranean keto” (olive oil, avocado, fish).
Saturated fats and LDL receptors
High intake of saturated fats (found in red meat, dairy, coconut oil) can downregulate LDL receptors in the liver. These receptors are responsible for clearing LDL from the bloodstream. When they are downregulated, LDL accumulates in the circulation, raising keto cholesterol levels. While saturated fat is not the villain it was once portrayed to be, some individuals are genetically hyper-absorbers of cholesterol or have specific ApoE genotypes (like ApoE4) that make them highly sensitive to dietary saturated fat.
Unsaturated fats and lipid improvement
Conversely, replacing saturated fats with monounsaturated fats (MUFAs) and polyunsaturated fats (PUFAs) has been shown to lower LDL cholesterol. A case study highlighted in clinical literature described a patient with the LMHR phenotype whose LDL dropped from 274 mg/dL to 111 mg/dL simply by switching fat sources from animal fats to unsaturated sources and slightly increasing carbohydrate intake, without medication.
How to do keto in a heart-healthy way
If you are committed to a low-carb lifestyle but are concerned about your keto heart health or have seen a rise in your lipid numbers, it is possible to adjust your diet to optimize your profile. We recommend a “heart-healthy” approach to keto that prioritizes nutrient density and lipid modulation.
Shift fat sources: fish over bacon
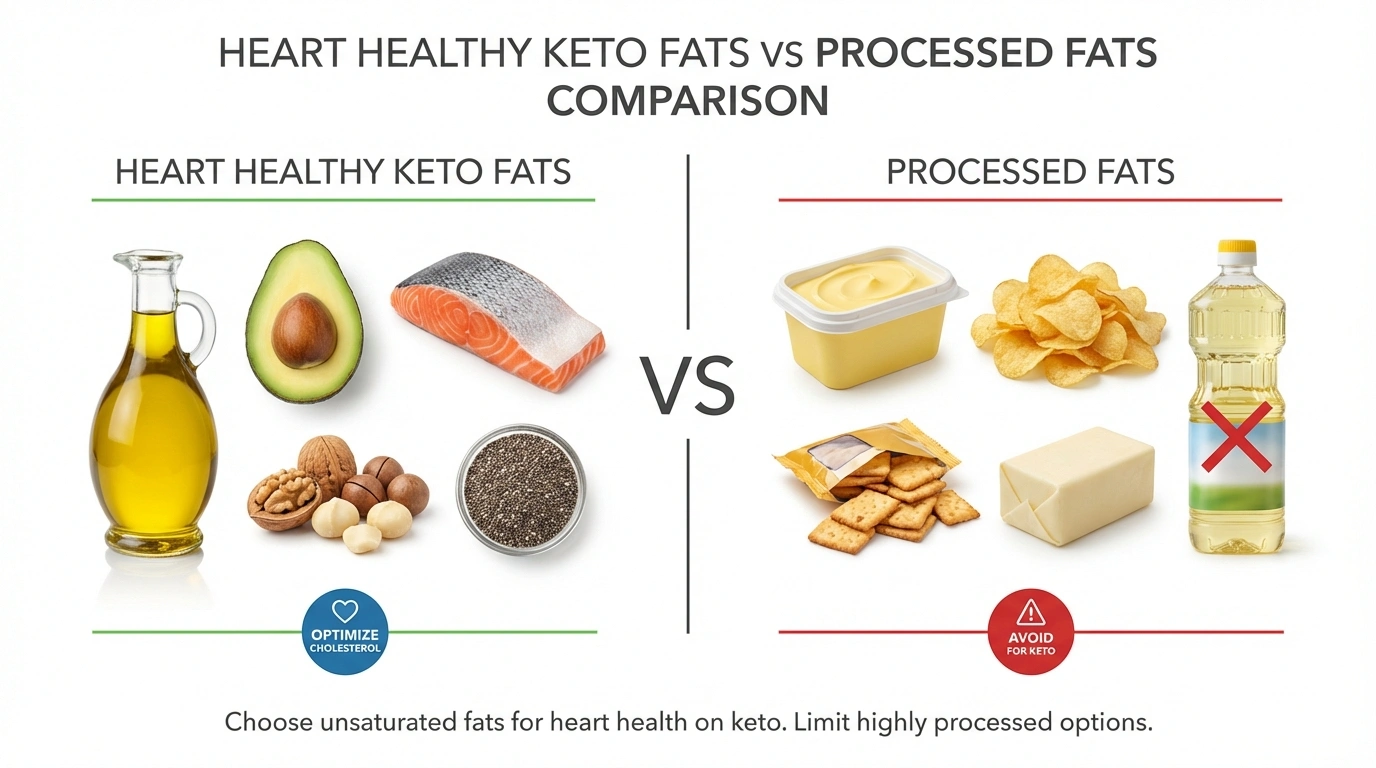
The most effective way to manage LDL keto diet elevations is to modify your fat intake:
- Reduce: butter, heavy cream, coconut oil, fatty cuts of beef, and processed meats (salami, bacon).
- Increase: extra virgin olive oil, avocado oil, avocados, macadamia nuts, walnuts, and fatty fish (salmon, mackerel, sardines) rich in omega-3s.
- Why: this increases the intake of monounsaturated fats, which are neutral or beneficial for LDL, and omega-3s, which help lower triglycerides and reduce inflammation.
Prioritize fiber-rich vegetables
A common mistake on keto is eliminating vegetables to keep carb counts low. However, low fiber intake can negatively impact the gut microbiome and cholesterol recycling:
- Strategy: eat ample amounts of low-carb, fibrous vegetables like broccoli, brussels sprouts, kale, spinach, and asparagus.
- Mechanism: soluble fiber binds to bile acids (made from cholesterol) in the gut and excretes them, forcing the liver to pull more LDL from the blood to make new bile.
- Gut health: fiber feeds beneficial gut bacteria (like bifidobacteria), which may play a role in regulating host lipid metabolism.
Avoid trans fats and processed keto foods
Many “keto-friendly” packaged snacks contain unhealthy fats or processed ingredients that can induce inflammation:
- Avoid: hydrogenated oils, soybean oil, and highly processed “keto bars.”
- Focus: whole, single-ingredient foods. Real food requires less label reading and offers better cardioprotection.
Incorporate plant sterols and stanols
Foods like nuts and seeds contain plant sterols that can compete with cholesterol for absorption in the digestive tract:
- Eat: almonds, chia seeds, flaxseeds, and hemp hearts. These are excellent sources of ALA (alpha-linolenic acid) and fiber.
Monitor labs regularly and advanced testing
Do not rely solely on a standard lipid panel. If you are on a ketogenic diet, request a more comprehensive analysis to assess true keto heart health:
- ApoB (apolipoprotein b): this measures the total number of atherogenic particles. It is a more accurate predictor of cardiovascular risk than LDL-C alone.
- LDL-P (LDL particle number): similar to ApoB, this counts the particles. Discordance (where LDL-C is normal but LDL-P is high) is a risk factor.
- CAC score (coronary artery calcium): a non-invasive scan that detects calcified plaque in the arteries. This measures actual disease presence rather than just risk factors.
Consider “mediterranean keto”
The mediterranean diet is widely considered the gold standard for heart health. Combining this with keto (ketotarian or mediterranean keto) offers the best of both worlds: the metabolic benefits of ketosis with the cardiovascular protection of plant-based fats and proteins. See common keto myths debunked for more info.
Interpreting your cholesterol results on keto
When you receive your lab results while in ketosis, interpretation requires a nuanced medical perspective. Here is a guide to understanding the numbers:
- High triglycerides (>150 mg/dL): this is unusual on keto. If yours are high, you may be consuming hidden carbs, drinking too much alcohol, or consuming excessive calories. It could also indicate that you are not actually in ketosis.
- Low HDL (<40 mg/dL men, <50 mg/dL women): this is a risk factor. To raise HDL, focus on exercise and consuming more olive oil and fish.
- High LDL (>160 mg/dL or >190 mg/dL):
- Scenario A: triglycerides are low (<100) and HDL is high (>60). This suggests you might be a hyper-responder. Discuss advanced testing (ApoB, CAC) with your doctor before starting statins, but do not ignore the elevation.
- Scenario B: triglycerides are high and HDL is low. This suggests “atherogenic dyslipidemia.” This is a dangerous profile. The diet is likely not working for you, or the quality of food is poor. Immediate adjustment is necessary.
Conclusion: is keto bad for your heart?
The question “is keto bad for heart health” does not have a universal answer. For patients with insulin resistance and type 2 diabetes, the ketogenic diet can be a powerful therapeutic tool that reduces cardiovascular risk factors like obesity, high blood sugar, and high triglycerides. However, for a subset of individuals, specifically those who respond with severe hypercholesterolemia, the diet requires modification.
Keto cholesterol elevations should not be dismissed as irrelevant, nor should they be cause for immediate panic. They are a signal to investigate further. By shifting from saturated to unsaturated fats, increasing fiber intake, and utilizing advanced lipid testing, most individuals can maintain the metabolic benefits of keto without compromising their cardiovascular future.
Disclaimer: this article is for informational purposes only and does not constitute medical advice. Lipid metabolism is complex and highly individual. Always consult with your healthcare provider or a lipidologist before making significant dietary changes or interpreting lab results, especially if you have a history of heart disease or familial hypercholesterolemia.
Explore More Resources
Further Reading & Tools
Understand how your body transitions to fat-burning mode.
Calculate your personal fat, protein, and carb limits.
Select the best fibrous veggies to support lipid health.