The definitive guide to ketogenic diet science: how your body transitions to ketosis
The ketogenic diet (KD), often referred to as the keto diet, is a metabolic strategy characterized by a very low intake of carbohydrates, moderate protein consumption, and high fat intake.
While recently popularized for rapid weight loss, the historical ketogenic diet science originated nearly a century ago as a therapeutic intervention for specific neurological conditions. Understanding the complex biochemistry behind how the body shifts its primary energy source—a state known as ketosis—is essential for safe and effective implementation. The fundamental principle driving the KD is the drastic reduction of carbohydrate intake, typically limiting consumption to less than 50 grams per day, and sometimes even less than 20–30 grams, depending on the individual. When the body is deprived of its typical fuel source (glucose), it is forced into a metabolic state where it begins breaking down stored fat into compounds called ketone bodies, which then serve as an alternative energy supply for the body and brain. This profound shift makes the ketogenic diet a powerful metabolic intervention.
Understanding metabolic shift: glucose vs. ketone metabolism
To appreciate the ketogenic diet science, one must first review basic cellular energy production. The human body generates energy in the form of adenosine triphosphate (ATP) through a process called cellular respiration, which primarily relies on glucose. This process involves three main stages: glycolysis, the tricarboxylic acid (TCA) cycle (Krebs cycle), and the electron transport chain.
Carbohydrates: the body’s preferred fuel source
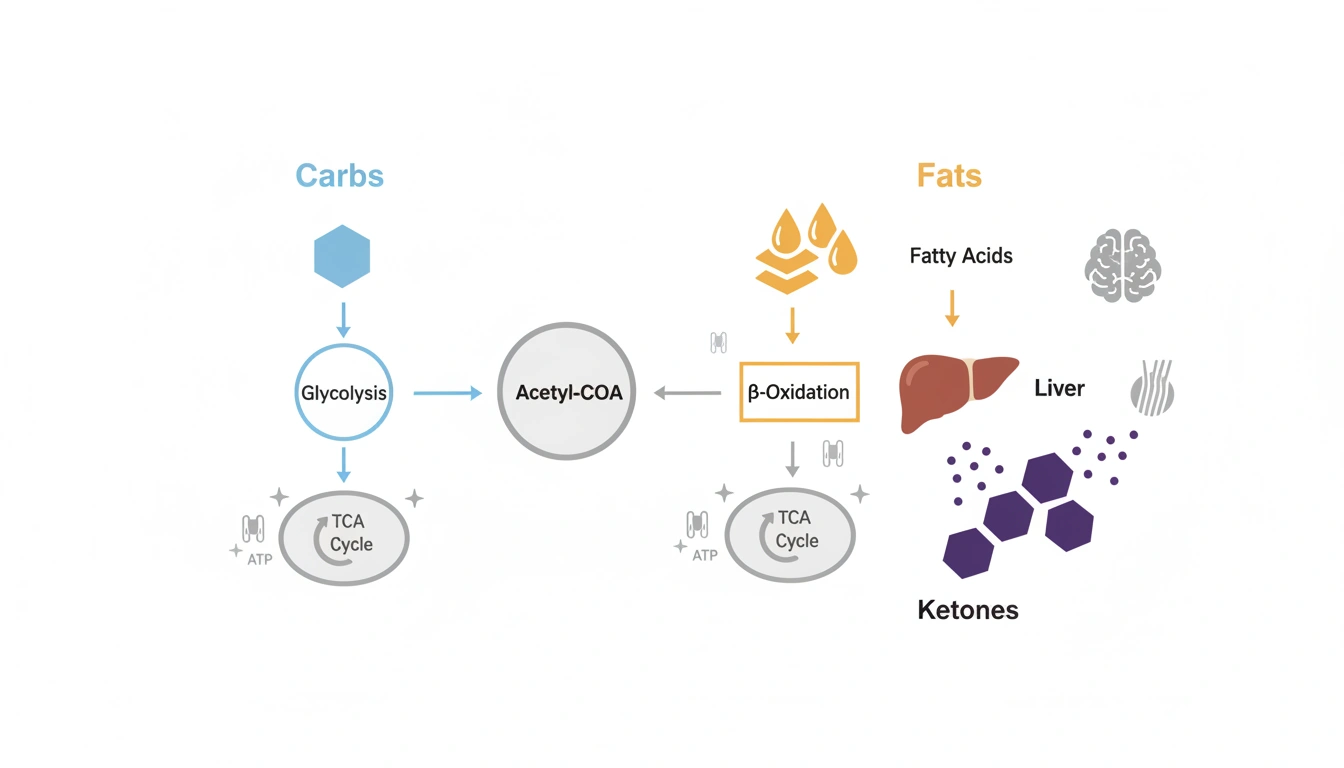
Under typical dietary conditions, carbohydrates are consumed and broken down into glucose, which is the primary and preferred metabolic substrate for most cells, including the liver and brain. Glucose molecules undergo glycolysis in the cell’s cytoplasm, producing pyruvate, which then enters the mitochondria to be converted into acetyl coenzyme A (acetyl-CoA). Acetyl-CoA subsequently enters the TCA cycle, culminating in the electron transport chain, where the bulk of ATP energy is generated.
Gluconeogenesis and glycogen depletion
When carbohydrate intake is severely restricted, the body’s easily accessible carbohydrate reserves, stored as glycogen in the liver, are rapidly depleted. Once these stores are exhausted, the body must produce its own glucose internally, primarily through a process called gluconeogenesis. Gluconeogenesis occurs mainly in the liver, using non-carbohydrate substrates such as pyruvate, lactic acid, glycerol, and specific amino acids (proteins). However, this endogenous glucose production is limited; proteins can only be converted to glucose by about 50%, and fats by only about 10% (due to their minimal glycerol content). This inability to rely heavily on fat for systemic glucose production means the body must find an alternative fuel source to satisfy the energy demands of organs like the brain.
Beta-oxidation: unleashing fat stores
When carbohydrates are scarce, the body enters a catabolic state, leading to the increased breakdown of fat, both dietary fat and stored triglycerides (adipose tissue). Triglycerides, composed of three fatty acids attached to a glycerol backbone, are broken down in the mitochondria by a process called beta-oxidation. Beta-oxidation directly generates acetyl-CoA. Since the body is low on carbohydrates, this acetyl-CoA bypasses the initial stages of glucose metabolism and is routed toward an alternative pathway in the liver—ketogenesis—to produce usable fuel.

The core mechanism: ketogenesis and ketone bodies
Ketosis is the metabolic state defined by an increased concentration of ketone bodies in the blood. This is the central tenet of ketogenic diet science.
The role of the liver in ketone production
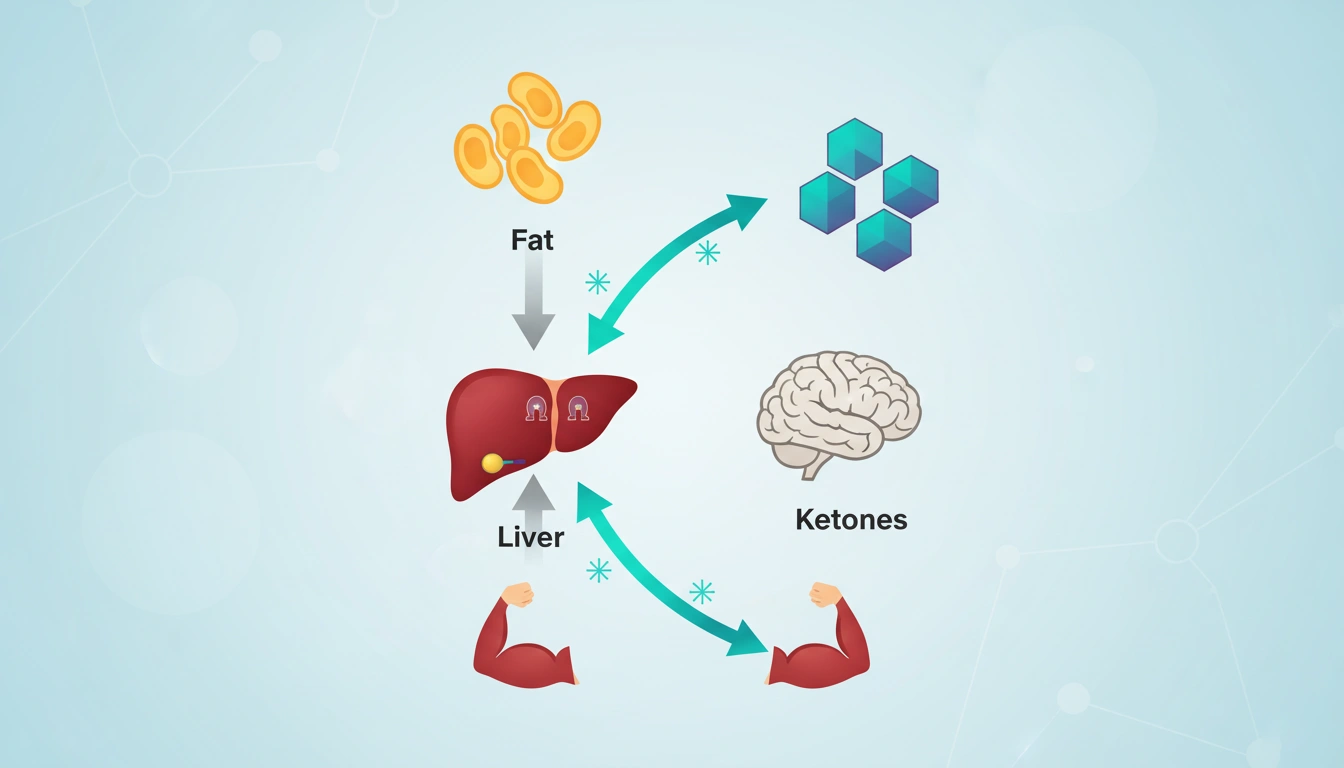
The liver is the primary site for the synthesis of ketone bodies, a process triggered by low insulin secretion and high levels of fatty acids resulting from limited carbohydrate intake. The acetyl-CoA generated from the breakdown of fatty acids is utilized by liver cells to synthesize these high-energy organic molecules.
The three principal ketone bodies
There are three primary ketone bodies produced during ketogenesis, which serve as crucial replacements for glucose:
- beta-hydroxybutyrate (BHB): the most abundant ketone body, found circulating in the blood. BHB is a carboxylic acid, though commonly referred to as a ketone body.
- acetoacetate: found in the urine.
- acetone: found in the breath, often causing the characteristic “keto” breath.
Ketone bodies, being water-soluble, can be transported through the bloodstream to various tissues. Vital organs such as the heart, muscle tissue, and kidneys can effectively use these synthesized ketone bodies for energy. Interestingly, the liver itself does not utilize ketones due to the lack of the necessary enzyme, diaphorase. Ketone bodies are often referred to as “super fuel” because they produce a greater amount of ATP compared to glucose. For instance, 100 grams of beta-hydroxybutyrate yields 10,500 grams of ATP, while 100 grams of glucose produces only 8,700 grams of ATP. This mechanism allows the body to maintain efficient fuel production even in a caloric deficit.
Nutritional ketosis vs. ketoacidosis: a critical distinction
A common misconception associated with the ketogenic diet science is the confusion between nutritional ketosis (a physiological state) and diabetic ketoacidosis (a pathological, life-threatening emergency).
- Nutritional Ketosis (Physiological): this state occurs due to fasting or a controlled, low-carbohydrate diet. Blood ketone levels typically range from 0.5 to 5 millimolar (mmol/L), with maximum levels reaching about 8 mmol/L. Importantly, in nutritional ketosis, blood pH remains normal, and the process is regulated by the small amount of insulin still present in the body.
- Diabetic Ketoacidosis (DKA) (Pathological): DKA is a severe complication, most often associated with uncontrolled type 1 diabetes (or prolonged alcoholism). DKA involves an uncontrolled, excessive buildup of ketones, leading to supra-physiological levels (15–25 mmol/L or even >20 mmol/L). This accumulation causes the blood pH to drop significantly (acidosis), requiring immediate medical attention.
In a healthy individual, life-threatening ketoacidosis cannot happen as long as the person can generate a small amount of insulin.
Physiological adaptation to ketosis: the keto-adaptive state
The body’s shift to utilizing ketones is a gradual process that takes time—at least a few weeks—known as keto-adaptation.
Fueling the brain: ketones cross the blood-brain barrier
The brain is an energetically demanding organ, and while it normally prefers glucose, it can adapt to use ketone bodies, particularly beta-hydroxybutyrate, when glucose is scarce. Under these low-carbohydrate conditions, ketone bodies can represent up to 75% of the brain’s total energy supply. The ability of ketones to cross the blood-brain barrier provides an alternative energy source for neurological function. This neuroprotective mechanism is partially why the ketogenic diet science has been historically applied to neurological disorders.
Effects on appetite and satiety
One of the key mechanisms contributing to weight loss on the KD is the effect on hunger and appetite.
- Satiety Hormones: the high fat and moderate protein content of the ketogenic diet promotes a greater feeling of satiety and fullness, which can lead to a spontaneous reduction in overall caloric intake.
- Ketone-Induced Anorexia: ketosis itself appears to provide a plausible explanation for the suppression of appetite. Research suggests that individuals adhering to the KD report less hunger and a reduced desire to eat.
Furthermore, the steady, low insulin levels achieved on the diet help reduce the sharp fluctuations that typically trigger hunger cues in the brain when following a high-carbohydrate diet.
New discoveries in ketone metabolism
Recent research has begun to uncover previously unrecognized complexity in how the body processes ketones. A collaborative study identified a metabolic “shunt pathway” where enzymes attach beta-hydroxybutyrate (BHB) to amino acids, producing a family of compounds called BHB-amino acids. This discovery suggests that ketones have active roles beyond simple fuel. The BHB-amino acids were found to chemically resemble Lac-Phe, a molecule known to suppress appetite after strenuous exercise. Consequently, these BHB-amino acids suppress feeding behaviors and promote weight loss, indicating that this “shunt pathway” is crucial for the regulation of appetite and ketosis-associated weight loss. The identification of these metabolites provides a new framework for investigating the mechanisms behind KD’s benefits, including seizure control.
Timeframe for keto-adaptation
The body’s shift from primarily burning glucose to efficiently utilizing fat and ketones is not instantaneous.
- Initial Entry: for most people, entering ketosis (detectable ketone levels) takes about 2 to 7 days of consuming less than 50 grams of carbohydrates daily.
- Adaptation: full keto-adaptation, where the body and brain efficiently use ketones for sustained energy, typically takes at least a few weeks.
- Factors Influencing Speed: individual factors such as age, metabolism, physical activity level, and previous diet (higher carb intake requires more time to deplete glycogen stores) influence how quickly ketosis is achieved. Intermittent fasting can also help speed up the process.
Clinical applications of ketogenic diet science
🧠 Epilepsy treatment: the historical foundation
The original therapeutic application of the ketogenic diet science was for the management of hard-to-control (refractory) epilepsy in children. Introduced in 1921 by Dr. Russell M. Wilder, the diet was designed to mimic the beneficial anti-convulsive effects observed during periods of fasting.
Efficacy: the KD remains an accepted therapeutic option for pharmaco-resistant epilepsy, particularly in children. Studies show that approximately half of patients who try the diet achieve a reduction in seizures of 50% or more, and about a third experience a reduction of over 90%. The effect can persist even after the diet is discontinued.
Specific Indications: KD is strongly considered for children who have failed to achieve seizure control with two or more anti-convulsant drugs. It is also a first-line therapy for certain metabolic diseases, such as pyruvate dehydrogenase (E1) deficiency and glucose transporter 1 deficiency syndrome (GLUT1-DS), which impair the body’s ability to use carbohydrates.
📈 Benefits for type 2 diabetes and insulin sensitivity
Due to its drastic limitation of carbohydrates, the ketogenic diet is highly effective in controlling blood sugar and improving metabolic health parameters.
Improved Glycemic Control: studies demonstrate that the KD can significantly improve insulin sensitivity, with one older study reporting an increase of 75%. This improvement, coupled with weight loss, helps lower blood sugar and the marker of long-term glucose control, hemoglobin A1c (HbA1c).
Reduced Medication Use: in individuals with type 2 diabetes, the KD has been shown to help decrease or eliminate the need for diabetes medications, always requiring close medical supervision for safe adjustment.
❤️ Impact on cardiovascular risk factors
The effects of the KD on cardiovascular health are complex and sometimes controversial, but potential benefits have been reported.
Lipid Profile Improvements (Short-Term): KD can positively impact lipid profiles by reducing triglyceride levels and increasing levels of high-density lipoprotein (HDL), often referred to as “good” cholesterol. Weight loss achieved on the diet may also help lower blood pressure.
LDL Concerns: conversely, some studies indicate a potential initial increase in low-density lipoprotein (LDL) cholesterol (the “bad” cholesterol), particularly when the diet is high in saturated fats, leading to concerns from organizations like the American College of Cardiology. This effect is not always maintained over the long term, but highlights the necessity of monitoring. Prioritizing healthy, unsaturated fats (like olive oil or fatty fish) is recommended to mitigate this risk.
🛡️ Neuroprotective potential in other conditions
Beyond epilepsy, the neuroprotective mechanisms of ketosis have prompted research into several other neurological and metabolic disorders.
Alzheimer’s and Parkinson’s disease: research suggests that ketones may help mitigate the neuroinflammation and oxidative stress often associated with neurodegenerative diseases like Alzheimer’s and Parkinson’s. By providing an alternative fuel source, KD may help palliate the hypometabolism suffered by neurons in these patients.
Other Conditions: KD is also being studied for potential therapeutic effects in polycystic ovarian syndrome (PCOS), by reducing insulin levels and improving androgen markers; traumatic brain injuries; and certain types of cancer (though research is inconclusive and often conflicting).
Types of ketogenic diets: macronutrient science
Standard ketogenic diet (SKD) and high-protein variants
The standard ketogenic diet (SKD) is the most extensively researched version and serves as the baseline for ketogenic diet science.
- Standard Ketogenic Diet (SKD): this is a very low-carb, moderate-protein, and high-fat diet. The typical ratio is approximately 70% fat, 20% protein, and 5%−10% carbohydrates.
- High-Protein Ketogenic Diet: this variant is similar to the SKD but increases the protein ratio, often to 60% fat, 35% protein, and 5% carbs.
The classic therapeutic ketogenic diet used for epilepsy typically follows a strict 4:1 ratio of fat weight to combined protein and carbohydrate weight, meaning 90% of calories come from fat.
Modified and targeted approaches
Other forms are typically used by athletes or individuals seeking greater flexibility.
- Modified Atkins Diet (MAD): does not restrict total calories or protein and has a lower overall ratio (approximately 1:1). It restricts carbohydrates initially to 10–20 grams per day.
- Cyclical Ketogenic Diet (CKD): this involves periods of high-carb refeeds, such as 5 ketogenic days followed by 2 high-carb days.
- Targeted Ketogenic Diet (TKD): allows for the addition of carbohydrates specifically around workout times.
- Medium-Chain Triglyceride (MCT) Diet: utilizes MCT oils (often derived from coconut oil) because they are more ketogenic than standard long-chain triglycerides (LCTs). This allows for a slightly higher allowance of protein and carbohydrates compared to the classic diet.
The importance of protein moderation
Maintaining moderate protein intake is crucial for sustaining nutritional ketosis.
- Preventing Gluconeogenesis: if protein consumption is too high (above roughly 35% of total calories or 1.0–1.5 grams per pound of lean body mass), the body can convert excess amino acids into glucose via gluconeogenesis. This rise in circulating glucose can interrupt the state of ketosis and reduce ketone levels.
- Kidney Strain: furthermore, excessive protein consumption forces the kidneys to excrete extra nitrogen, potentially straining individuals with pre-existing kidney conditions.
Dietary compliance: foods to embrace and avoid
Meals should be based predominantly on whole, high-fat, and moderate-protein sources:
Foods to prioritize (high fat, low carb)
- Healthy Oils and Fats: olive oil, coconut oil, avocado oil, butter, cream, and ghee.
- Fatty Proteins: red meat, pork, ham, bacon, poultry, eggs (ideally pasture-raised or omega-3 enriched), and fatty fish (salmon, trout, mackerel, herring).
- Dairy (High Fat): unprocessed cheeses (cheddar, mozzarella, blue, cream), sour cream, and full-fat greek yogurt.
- Nuts and Seeds: almonds, walnuts, flaxseeds, chia seeds, and pumpkin seeds.
- Low-Carb Vegetables: leafy greens (spinach, kale, arugula), cruciferous vegetables (broccoli, cauliflower, brussels sprouts), asparagus, zucchini, bell peppers, tomatoes, and mushrooms.
- Low-Carb Fruits (in strict moderation): berries (strawberries, raspberries, blackberries) and avocado.
Foods to severely limit or eliminate (high carb)
To maintain ketosis, virtually all foods high in carbohydrates must be restricted.
- Sugars and Sweets: soda, fruit juices, smoothies, candy, ice cream, cake, and any other sugary drinks or foods.
- Grains and Starches: wheat-based products (bread, pasta), rice, oatmeal, cereals, and other grains.
- Starchy Vegetables and Tubers: potatoes, sweet potatoes, parsnips, carrots, and corn.
- Legumes: peas, beans, lentils, and chickpeas.
- Most Fruits: all high-sugar fruits (e.g., bananas, apples, grapes, mango) are restricted.
- Processed Foods: most diet or low-fat products, processed vegetable oils, and high-sugar condiments (ketchup, BBQ sauce).
Risks and necessary medical monitoring in ketogenic diet science
🤒 Navigating short-term side effects: the “keto flu”
As the body transitions into ketosis, individuals commonly experience the “keto flu,” a cluster of symptoms that usually last from a few days up to two to four weeks. Common symptoms include:
- Fatigue and Low Energy: often attributed to the body’s struggle to adapt to fat as the primary fuel source.
- Headaches and Brain Fog: poor mental function and difficulty concentrating are frequently reported.
- Gastrointestinal Distress: nausea, vomiting, diarrhea, and constipation are common.
- Electrolyte Imbalance: the initial rapid weight loss is often water weight (due to glycogen depletion), which flushes out electrolytes. This loss can cause muscle cramps and dehydration.
Mitigation strategies:
- Hydration and Electrolytes: increasing water intake and replenishing electrolytes (sodium, potassium, magnesium) is crucial to alleviate symptoms. Recommended mineral intake includes 3,000–4,000 mg of sodium, 1,000 mg of potassium, and 300 mg of magnesium daily, especially in the beginning.
- Gradual Initiation: slowly lowering carbohydrate consumption over a few weeks can help the body adjust more smoothly.
🩺 Long-term nutritional and organ health considerations
Long-term adherence to a KD, especially when unsupervised, raises significant concerns:
- Nutrient Deficiencies: because the diet severely restricts whole grains, legumes, and many fruits and vegetables, there is a risk of deficiencies in essential micronutrients, including vitamin D, calcium, b vitamins (thiamine/B1, folate), iron, and magnesium. Supplementation is necessary to counteract these dietary limitations.
- Kidney Health and Stones: the KD increases the risk of kidney stones (nephrolithiasis) due to several factors, including acidosis (which increases bone demineralization and calcium excretion), hypocitraturia (low citrate concentration), and low urine pH. People with pre-existing kidney insufficiency should not be on a high-protein diet as it can exacerbate their condition.
- Cardiovascular Risk: sustained high intake of saturated fats and animal products (often favored on keto) is associated with an increased risk of heart disease and may worsen lipid profiles by increasing LDL cholesterol.
- Liver Function: people with pre-existing liver conditions may metabolize excess fat poorly, and the diet can exacerbate these underlying issues. Hepatic steatosis (extra fat in the liver) is a reported long-term adverse effect.
- Potential Accelerated Aging (Controversial Study): a study conducted on mice suggested that long-term, sustained KD might accelerate the aging of vital organs (heart, liver, and brain) by inducing cellular senescence (the accumulation of non-dividing “zombie cells” that release inflammatory substances) through the activation of the tumor suppressor gene p53. However, the same research showed that this aging effect was reversible upon switching back to a standard diet, and an intermittent KD schedule (4 days keto, 7 days standard) did not increase p53 activation or cellular senescence.
🚫 Contraindications and the need for professional supervision
The ketogenic diet science confirms that this regimen is not universally suitable. Consultation with a physician or specialized registered dietitian is mandatory before initiation, especially for those with underlying health conditions. The KD is strictly contraindicated for individuals with:
- Pancreatitis.
- Liver failure or cirrhosis.
- Disorders of fatty acid oxidation or fat metabolism (e.g., carnitine deficiencies, porphyrias, pyruvate kinase deficiency).
- Uncontrolled metabolic or homeostatic disorders.
- Individuals taking SGLT2 inhibitors for type 2 diabetes, due to the increased risk of diabetic ketoacidosis (DKA).
- Children (except for specific medical indications like refractory epilepsy or metabolic disorders).
- Pregnancy and lactation.
Ketogenic diet science and weight management efficacy
Weight reduction on a KD is driven by multiple factors:
- Increased fat burning (ketosis): by drastically limiting glucose, the body is forced to increase the metabolism of stored fat for energy.
- Diuretic effect: the initial rapid weight loss (often 2–3 kg in the first few days) is largely water weight lost as stored glycogen reserves are depleted.
- Appetite suppression: the high fat/protein content and the presence of ketones reduce hunger and lead to a spontaneous reduction in caloric intake, which is critical for weight loss.
- Metabolic expenditure: the body expends a significant amount of energy (caloric expenditure) converting fats and proteins into necessary glucose (gluconeogenesis), contributing to weight loss.
Short-term vs. long-term results
Studies consistently show that the KD leads to faster initial weight loss compared to traditional low-fat or even Mediterranean diets. A meta-analysis comparing very low-carbohydrate KD to low-fat diets found superior weight reduction with KD in the long term. However, this advantage often diminishes over extended periods. Many experts caution that the highly restrictive nature of the KD makes long-term adherence difficult, leading to potential “yo-yo dieting,” which is associated with increased mortality. A Mediterranean-style diet, which is rich in fruits, vegetables, whole grains, and quality fats like olive oil, mixed with intermittent fasting, is often advised for the greatest longevity and lowest risk of heart disease.
Implementation and monitoring: ensuring safety
Required professional team
Safe implementation of the KD involves an interprofessional healthcare team:
- Physician/Neurologist: to screen for contraindications, monitor underlying conditions (especially heart and kidney health), and adjust medications (critical for diabetes patients).
- Registered Dietitian (RD): to calculate the precise macronutrient ratios (ketogenic ratio, calorie needs, fluid intake), customize meal plans, and monitor for nutritional deficiencies.
- Pharmacist: to advise on the carbohydrate content of necessary medications and supplements.
Monitoring ketosis
The physiological state of ketosis can be monitored to ensure the diet is effectively restricting carbohydrates and converting fat into fuel.
- Testing Methods: ketones can be measured in the blood (most accurately, focusing on beta-hydroxybutyrate), urine (using nitroprusside strips for acetoacetate), or breath (for acetone excretion).
- Blood Monitoring: blood ketone levels between 1.5 and 3.0 mmol/L are often considered the optimal ketosis range for desired effects.
- Regular Clinical Labs: regular analysis of the lipid status (total cholesterol, HDL, LDL, triglycerides), as well as monitoring renal and hepatic function, is crucial for long-term safety.
Conclusion: the power and precision of ketogenic diet science
The ketogenic diet is a profound metabolic intervention rooted in solid ketogenic diet science, originally developed for therapeutic use in epilepsy. By severely restricting carbohydrates, the body successfully transitions from burning glucose to relying on fat and the subsequent production of ketone bodies (nutritional ketosis). These ketones serve as a highly efficient “super fuel” for both the body and the brain, driving rapid short-term weight loss, improving glucose control and insulin sensitivity, and offering neuroprotective benefits. However, the power of the ketogenic diet comes with inherent risks, including the potential for nutrient deficiencies, kidney stone formation, and long-term cardiovascular concerns, particularly if the diet is high in poor-quality saturated fats. Due to its highly restrictive nature and complex metabolic impact, the KD is not a casual or sustainable long-term solution for the general population. It is imperative that anyone considering a ketogenic diet consults with a specialized healthcare professional, such as a physician and a registered dietitian, to ensure that the diet is medically appropriate for their individual health status and that proper nutritional and metabolic monitoring is maintained.
Explore More Keto Science & Diet Resources
For additional information, clinical studies, and comprehensive guides on ketogenic diet science, check out these excellent resources: